|
Overview
 Fallen arches shouldn?t (if possible) be confused with feet that are normally flat. Arch height varies a lot from individual to individual. If you have fairly flat feet, but notice that an arch appears when you stand on your tiptoes (flexible flatfoot), and if you don?t experience any pain with your flat feet, you?re more likely to be okay. However, if your feet still fail to arch when up on your toes, if your feet lose an arch you used to have, or if you experience any painful symptoms, you probably ought to see a podiatrist. Causes Some people develop fallen arches because they tend to pronate, or roll inwards on the ankles, says the Instep Foot Clinic. Other people may simply have under-developed muscles in their arches. Your arches help your feet bear weight and are supported in this job by muscles and tendons in your feet and ankles. So, while fallen arches aren?t usually serious, they can cause pain in your feet, ankles, knees and/or hips due to your reduced weight-bearing ability. In these cases, treatment may be required. Orthotics that sit in your shoes and support your arches are a common solution, as are exercises to strengthen and stretch your feet and leg muscles. Symptoms Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles. Diagnosis If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma. Can you fix a fallen arch? Non Surgical Treatment If the condition is not bothering you or preventing you from being mobile, you may not need treatment (depending on your doctor?s diagnosis). Generally, treatment is reserved for those who have additional problems. Still, your doctor will probably recommend a simple treatment plan for your condition. This treatment may include rest and icing the arch, changing footwear, anti-inflammatory medication, using orthotics, over-the-counter medication such as ibuprofen, physical therapy. Corticosteroid injection (usually used in cases of severe pain). If these methods do not relieve symptoms of flat feet, your doctor may recommend surgery to reduce pain and improve the alignment of your bones. Surgical Treatment  This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients. Prevention Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches. Overview
If one scans the literature it readily becomes obvious that leg length discrepancy/asymmetry is a common finding. This fact has been a very controversial topic within chiropractic, and diagnostic rationales have been built around this very common finding. The object of this column is to consider some of the causes of this discrepancy that the profession may have ignored or not been aware of.  Causes Some causes of leg length discrepancy (other than anatomical). Dysfunction of the hip joint itself leading to compensatory alterations by the joint and muscles that impact on the joint. Muscle mass itself, i.e., the vastus lateralis muscle, pushes the iliotibial band laterally, causing femoral compensations to maintain a line of progression during the gait cycle. This is often misdiagnosed as I-T band syndrome and subsequently treated incorrectly. The internal rotators of the lower limb are being chronically short or in a state of contracture. According to Cunningham's Manual of Practical Anatomy these are muscles whose insertion is lateral to the long axis of the femur. The external rotators of the hip joint are evidenced in the hip rotation test. The iliosacral joint displays joint fixations on the superior or inferior transverse, or the sagittal axes. This may result from many causes including joint, muscle, osseous or compensatory considerations. Short hamstring muscles, i.e., the long head of the biceps femoris muscle. In the closed kinetic chain an inability of the fibula to drop inferior will result in sacrotuberous ligament loading failure. The sacroiliac joint dysfunctions along its right or left oblique axis. Failure or incorrect loading of the Back Force Transmission System (the longitudinal-muscle-tendon-fascia sling and the oblique dorsal muscle-fascia-tendon sling). See the proceedings of the first and second Interdisciplinary World Congress on Low Back Pain. Sacral dysfunction (nutation or counternutation) on the respiratory axis. When we consider the above mentioned, and other causes, it should be obvious that unless we look at all of the causes of leg length discrepancy/asymmetry then we will most assuredly reach a diagnosis based on historical dogma or ritual rather than applying the rules of current differential diagnosis. Symptoms Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down. Diagnosis Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all. Non Surgical Treatment Treatment depends on what limb has the deformity and the amount of deformity present. For example, there may be loss of function of the leg or arm. Cosmetic issues may also be a concern for the patient and their family. If there are problems with the arms, the goal is to improve the appearance and function of the arm. Treatment of leg problems try to correct the deformity that may cause arthritis as the child gets older. If the problem is leg length, where the legs are not "equal," the goal is equalization (making the legs the same length). Treatment may include the use of adaptive devices, prosthesis, orthotics or shoe lifts. If the problem is more severe and not treatable with these methods, then surgery may be necessary.  how to increase height after 25 Surgical Treatment Differences of an inch-and-a-half to two inches may require epiphysiodesis (adjusting the growth of the longer side) or acute shortening of the other side. Differences greater than 2.5 inches usually require a lengthening procedure. The short bone is cut and an external device is applied. Gradual lengthening is done over months to allow the muscles and nerves accommodate the new length. Overview
 The most common cause of heel pain is plantar fasciitis which is commonly referred to as a heel spur. Plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, from the heel to the toes. Plantar fasciitis is a condition in which the plantar fascia is inflamed. This condition can be very painful and cause a considerable amount of suffering. Causes Heel pain has many causes. Heel pain is generally the result of faulty biomechanics (walking gait abnormalities) that place too much stress on the heel bone and the soft tissues that attach to it. The stress may also result from injury, or a bruise incurred while walking, running, or jumping on hard surfaces; wearing poorly constructed footwear (such as flimsy flip-flops); or being overweight. Symptoms Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain. Diagnosis A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem. Non Surgical Treatment Once diagnosed, treatment for plantar fasciitis may include one or more of the following: advice on footwear, in particular use of arch-supportive footwear; avoid walking barefoot; stretching exercises, shoe modifications such as heel pads, taping and strapping, anti-inflammatories and orthotic devices to correct abnormal foot mechanics. Injection therapy with corticosteroids is only advisable if all the conservative treatment methods mentioned above have been exhausted due to undesired effects implicated with steroid infusion in the heels. Surgical Treatment If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. how to get rid of heel spurs Prevention  Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs. Overview
Have you noticed that your pants always fit a little weird or that you are always leaning to one leg when standing for awhile? If so, one of your legs may be longer than the other. This is known as a leg length discrepancy. There are two main reasons for a leg length discrepancy. One reason is that one of your leg bones (tibia or femur) is longer on one side. This is referred to as a true leg length discrepancy because the actual length of your bones is different. A second reason is that your pelvic bone may be rotated on one side making it appear that one leg is longer than the other. This is referred to as an apparent leg length discrepancy because the actual length of your leg bones is not different. In order to figure out if you have a true or apparent leg length discrepancy, your doctor may take an x-ray to measure the length of your leg bones or a simple measurement from your belly button to your ankle can help determine the reason. Over time, the leg length difference can cause stress on your low back, hips and knees, which may cause pain or discomfort.  Causes There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities. Symptoms The patient/athlete may present with an altered gait (such as limping) and/or scoliosis and/or low back pain. Lower extremity disorders are possibly associated with LLD, some of these are increased hip pain and degeneration (especially involving the long leg). Increased risk of: knee injury, ITB syndrome, pronation and plantar fascitis, asymmetrical strength in lower extremity. Increased disc or vertebral degeneration. Symptoms vary between patients, some patients may complain of just headaches. Diagnosis The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used. Non Surgical Treatment The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.  how can a woman look taller? Surgical Treatment The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed. Overview
 Morton?s Neuroma is a common foot condition characterized by pain and swelling in the ball of the foot, between the third and fourth toes. It?s caused by bones in your feet squeezing a nerve. Symptoms include a sharp, burning pain and possibly separation between the affected toes. Morton?s Neuroma is a common foot condition characterized by pain and swelling in the ball of the foot, between the third and fourth toes. It?s caused by bones in your feet squeezing a nerve. Symptoms include a sharp, burning pain and possibly separation between the affected toes.Causes There are orthoses and corrective shoes that can effectively alleviate disturbances to foot mechanics. A podiatric physician can prescribe the best corrective footwear and shoe inserts for all activities, work, exercise, play, walking, shopping and more, based on an analysis of the patient?s foot and his or her lifestyle. Improper footwear. Podiatric physicians have long believed that constricting, narrow, poor-fitting shoes with a tight or pointed toe box tend to compress the end of the foot, leading to abnormal motion of the foot and to excessive pressure in the area of the nerve. High-heeled shoes are a particular culprit here, since they put pressure on the area around wearer?s toes and the ball of the foot. Symptoms Many patients describe the sensation as a burning pain in the ball of the foot that often radiates to the toes. Initially, the pain may become much more apparent when the person wears tight, narrow or high-heeled shoes, or engages in activities which place pressure on the foot. Eventually, symptoms may be continuous and last for days, and even weeks. MRI (magnetic resonance imaging) scans have revealed Morton's neuroma lesions in patients who had no symptoms at all. Symptoms can become so disrupting that many affected individuals become anxious about walking, or even placing their foot on the ground. Diagnosis Plain x-rays of the foot may demonstrate that one or more of the metatarsals are long (Figure #5). Not uncommonly, the second and/or third metatarsal may be long relative to the third or fourth. This can create a situation where excessive load is occurring in and around the vicinity of the interdigital nerve. Non Surgical Treatment Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.  Surgical Treatment If conservative treatments haven't helped, your doctor might suggest injections. Some people are helped by the injection of steroids into the painful area. In some cases, surgeons can relieve the pressure on the nerve by cutting nearby structures, such as the ligament that binds together some of the bones in the front of the foot. Surgical removal of the growth may be necessary if other treatments fail to provide pain relief. Although surgery is usually successful, the procedure can result in permanent numbness in the affected toes. Prevention Women, particularly those who wear tight shoes, are at greatest risk for Morton?s neuroma. The best way to prevent the condition is to wear shoes with wide toe boxes. Tight, pointed shoes squeeze bones, ligaments, muscles and nerves. High heels may worsen the problem by shifting your weight forward. Over time, this combination can cause the nerves to swell and become painful.  Overview OverviewA Hammertoes or contracted toe is a deformity of the proximal interphalangeal joint of the second, third, or fourth toe causing it to be permanently bent, resembling a hammer. Mallet toe is a similar condition affecting the distal interphalangeal joint. Causes Hammertoes are more commonly seen in women than men, due to the shoe styles women frequently wear: shoes with tight toe boxes and high heels. Genetics plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities of the feet, such as flat feet and feet with abnormally high arches. These biomechanical abnormalities cause the muscles and tendons to be used excessively or improperly, which deforms the toes over time.  Symptoms The most obvious sign of hammertoes are bent toes, other symptoms may include pain and stiffness during movement of the toe. Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box. Painful calluses on the bottoms of the toe or toes. Pain on the bottom of the ball of the foot. Redness and swelling at the joints. Diagnosis Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred. Non Surgical Treatment Mild hammer toe in children can be treated by manipulating and splinting the affected toe. The following changes in footwear may help relieve symptoms. Wear the right size shoes or shoes with wide toe boxes for comfort, and to avoid making hammer toe worse. Avoid high heels as much as possible. Wear soft insoles to relieve pressure on the toe. Protect the joint that is sticking out with corn pads or felt pads. A foot doctor can make foot devices called hammer toe regulators or straighteners for you, or you can buy them at the store. Exercises may be helpful. You can try gentle stretching exercises if the toe is not already in a fixed position. PIcking up a towel with your toes can help stretch and straighten the small muscles in the foot. Surgical Treatment If these treatments are not sufficient at correcting the hammer toe, an operation to straighten the toe may be necessary. This is often performed in conjunction with surgery for a bunion deformity. The surgical treatment of a hammer toe can consist of either cutting the tendons to relieve the pressure that causes the deformity, or fusing the toe so that it points straight permanently.  Prevention The best ways to prevent a hammertoe are. Wear shoes that fit well. Shoes should be one-half inch longer than your longest toe. Shoes should be wide enough and the toe box should be high enough to give the foot room to move. Don?t wear shoes with heels over 2 inches high. If a toe starts to look like a hammertoe, buy shoes that have an extra high toe box. Wear corn pad removers or cushion pads on top of the affected toe. See your healthcare provider any time you have foot pain that does not go away quickly or is more than mild pain. Foot pain is not normal.  Overview OverviewHammertoe is a condition in which the toes of your feet become contracted into an upside-down "V" shape, causing pain, pressure and, often, corns and calluses. Hammer Toe can develop on any of the toes, but generally affects the middle three toes, most often the second toe. The bones, muscles, ligaments and tendons of your feet normally are well-balanced to distribute your body's weight while standing, walking and running. When the first and second joints of your toes experience the prolonged stress that develops when the muscles that control them fail to work together properly, the pressure on the tendons that support them can lead to the curling or contraction known as hammertoe. Causes Hammertoe and mallet toe have been linked to certain shoes. High-heeled shoes or footwear that's too tight in the toe box can crowd your toes into a space that's not large enough for them to lie flat. This curled toe position may eventually persist even when you're barefoot. Trauma. An injury in which you stub, jam or break a toe may make it more likely for that digit to develop hammertoe or mallet toe. Nerve injuries or disorders. Hammertoe and mallet toe are more common in people who have nerve damage in their feet, which often occurs with such medical problems as a stroke or diabetes.  Symptoms Common reasons patients seek treatment for toe problems are toe pain on the knuckle. Thick toe calluses. Interference with walking/activities. Difficulty fitting shoes. Worsening toe deformity. Pain at the ball of the foot. Unsightly appearance. Toe deformities (contractures) come in varying degrees of severity, from slight to severe. The can be present in conjunction with a bunion, and develop onto a severe disfiguring foot deformity. Advanced cases, the toe can dislocate on top of the foot. Depending on your overall health, symptoms and severity of the hammer toe, the condition may be treated conservatively and/or with surgery. Diagnosis Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. Non Surgical Treatment Conservative treatment is the first choice, often starting with a change of shoes to ones that have soft, larger toe spaces. Toe exercises may be prescribed to stretch and strengthen the toe muscles. Over-the-counter straps, cushions or non-medicated corn pads may be recommended to help relieve your symptoms. Surgical Treatment Surgery may be the treatment of choice if conservative approaches prove unsuccessful. Usually performed as an outpatient procedure, the specific surgery will depend on the type and extent of injury to the toe. Recovery my take several days or weeks and you may experience some redness, stiffness and swelling of the affected toe. Your physician will recommend taking it easy and to keep your foot elevated while you recover.  Prevention These tips may help you buy the right shoes. Buy shoes at the end of the day. Your feet are smaller in the morning and swell throughout the day. Don't assume your shoe size hasn't changed. As you age, your shoe size may change, especially the width. Measure both feet and buy for the larger foot. Ask for just the right fit. A shoe repair store can stretch shoes in tight spots.  Overview OverviewHammer, claw, and mallet toes are toes that do not have the right shape. They may look odd or may hurt, or both. Tight shoes are the most common cause of these toe problems. A hammertoe is a toe that bends down toward the floor at the middle toe joint. It usually happens in the second toe. This causes the middle toe joint to rise up. Hammer toes often occur with bunions. Claw toe often happens in the four smaller toes at the same time. The toes bend up at the joints where the toes and the foot meet. They bend down at both the middle joints and at the joints nearest the tip of the toes. This causes the toes to curl down toward the floor. A mallet toe often happens to the second toe, but it may happen in the other toes as well. The toe bends down at the joint closest to the tip of the toe. Causes People who are born with long bones in their toes are more likely to develop hammer toe. Children who wear shoes they have outgrown may develop this condition. People who wear very narrow shoes or high-heeled shoes are also more likely to develop a hammer toe. Sometimes, pressure from a bunion can cause hammer toe. Rheumatoid arthritis is another a risk factor.  Symptoms SymptomsThe most obvious symptom of hammer, claw or mallet toe is the abnormal toe position. This is usually combined with pain: the abnormal foot position leads to excessive friction on the toe as it rubs against any footwear which can be extremely painful. Corns & Calluses: repeated friction can result in the formation of a foot corn or callus on top of the toes. Stiffness, the joints become increasingly stiff. In the early stages, the toes can usually be straightened out passively using your hands, but if allowed to progress, the stiffness may be permanent. Diagnosis Some questions your doctor may ask of you include, when did you first begin having foot problems? How much pain are your feet or toes causing you? Where is the pain located? What, if anything, seems Hammer toes to improve your symptoms? What, if anything, appears to worsen your symptoms? What kind of shoes do you normally wear? Your doctor can diagnose hammertoe or mallet toe by examining your foot. Your doctor may also order X-rays to further evaluate the bones and joints of your feet and toes. Non Surgical Treatment If your hammertoe problem is diagnosed as flexible hammertoe, there are a number of nonsurgical treatments that may be able to straighten out your toe or toes and return them to their proper alignment. Padding and Taping. Your physician may pad the boney top-part of your hammertoe as a means of relieving pain, and may tape your toes as a way to change their position, correct the muscle imbalance and relieve the pressure that led to the hammertoe's development. Medication. Anti-inflammatory drugs such as aspirin and ibuprofen can help deal with inflammation, swelling and pain caused by your hammertoe. Cortisone injections may be prescribed for the same purpose. If your hammertoe is a consequence of arthritis, your physician may prescribe medications for that. Surgical Treatment If these treatments are not sufficient at correcting the hammer toe, an operation to straighten the toe may be necessary. This is often performed in conjunction with surgery for a bunion deformity. The surgical treatment of a hammer toe can consist of either cutting the tendons to relieve the pressure that causes the deformity, or fusing the toe so that it points straight permanently. Overview
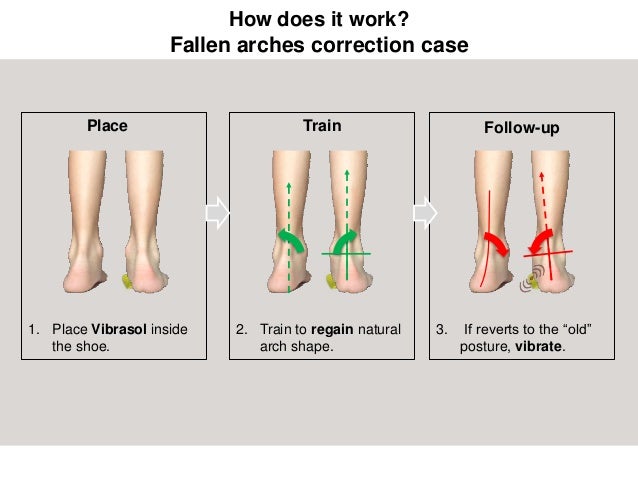
Over Pronation (Flat Feet) refers to the biomechanical shock-absorbing motion of the ankle, foot and lower leg. It is the natural inward flexing motion of the lower leg and ankle. Standing, walking, and running cause the ankle joint to pronate which in turn helps the body to absorb shock and allows it to control balance. An ankle joint that is too flexible causes more pronation than desired. This common condition is called Over- Pronation (sometimes referred to as "Flat Feet"). This foot condition places an extreme degree of strain on various connective tissues of the ankle, foot, and knee. If this condition is not addressed foot pain and toe deformities such as bunions and hammer toes (just to name a couple) may develop. Hip and lower back pain may also be residual results from this condition.  Causes There are many possible causes for overpronation, but researchers have not yet determined one underlying cause. Hintermann states, Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles. Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe. Symptoms With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs. Diagnosis People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.  Non Surgical Treatment Although there is no actual cure for over-pronation it is possible to correct or at least reduce this problem. In order to restore our normal foot function an 'orthotic' or orthotic insole device is placed inside the shoes. Orthotics are designed to realign the foot and ankle bones to their natural position. This in turn restores our normal foot function and it helps alleviate not only foot problems but also ailments in other parts of the body i.e. the legs, knees and lower back. In addition to wearing an orthotic, it is recommended to wear supportive shoes, like good quality athletic footwear with a firm heel counter and sufficient flexibility in the forefoot area. Prevention Many of the prevention methods for overpronation orthotics, for example, can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function. Overview
Sever's disease is the most common cause of heel pain in the growing child. It is due to overuse and repetitive stress of the Achilles tendon where it attaches to the heel bone. Causes This condition most commonly occurs due to repetitive or prolonged activities placing strain on the heel's growth plate, typically during a period of rapid growth. These activities (or sports) usually involve excessive walking, running, jumping or hopping. Severs disease may also be more likely to occur following a poorly rehabilitated sprained ankle, in patients with poor foot biomechanics or those who use inappropriate footwear. In young athletes, this condition is commonly seen in running and jumping sports, such as football, basketball, netball and athletics. Symptoms The most prominent symptom of Sever's disease is heel pain which is usually aggravated by physical activity such as walking, running or jumping. The pain is localized to the posterior and plantar side of the heel over the calcaneal apophysis. Sometimes, the pain may be so severe that it may cause limping and interfere with physical performance in sports. External appearance of the heel is almost always normal, and signs of local disease such as edema, erythema (redness) is absent. The main diagnostic tool is pain on medial- lateral compression of the calcaneus in the area of growth plate, so called squeeze test. Foot radiographs are usually normal. Therefore the diagnosis of Sever's disease is primarily clinical. Diagnosis You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate. Non Surgical Treatment Sever?s disease is believed to be the byproduct of repepitive stress and trauma to the growth plate in the calcaneous, or heel bone. The stress is from the pull of the Achilles tendon on the growth plate where the tendon attaches. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
July 2017
Categories |
 RSS Feed
RSS Feed
