|
Overview
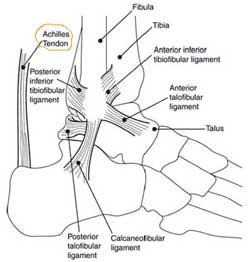 The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight. Causes An Achilles tendon rupture is often caused by overstretching the tendon. This typically occurs during intense physical activity, such as running or playing basketball. Pushing off from the foot while the knee is straight, pivoting, jumping, and running are all movements that can overstretch the Achilles tendon and cause it to rupture. A rupture can also occur as the result of trauma that causes an over-stretching of the tendon, such as suddenly tripping or falling from a significant height. The Achilles tendon is particularly susceptible to injury if it is already weak. Therefore, individuals who have a history of tendinitis or tendinosis are more prone to a tendon rupture. Similarly, individuals who have arthritis and overcompensate for their joint pain by putting more stress on the Achilles tendon may also be more susceptible to an Achilles tendon rupture. Symptoms Symptoms of an Achilles tendon injury are as follows. Pain along the back of your foot and above your heel, especially when stretching your ankle or standing on your toes; with tendinitis, pain may be mild and worsen gradually. If you rupture the tendon, pain can be abrupt and severe. Tenderness. Swelling. Stiffness. Hearing a snapping or popping noise during the injury. Difficulty flexing your foot or pointing your toes (in complete tears of the tendon). Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment This condition should be diagnosed and treated as soon as possible, because prompt treatment probably improves recovery. You may need to be referred urgently to see a doctor in an orthopaedic department or accident and emergency department. Meanwhile, if a ruptured Achilles tendon is suspected, you should not put any weight on that foot, so do not walk on it at all.Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. The decision of whether to proceed with surgery or non-surgical treatment is based on the severity of the rupture and the patient?s health status and activity level. Non-surgical treatment, which is generally associated with a higher rate of re-rupture, is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. Non-surgical treatment involves use of a cast, walking boot, or brace to restrict motion and allow the torn tendon to heal. The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight. Causes An Achilles tendon rupture is often caused by overstretching the tendon. This typically occurs during intense physical activity, such as running or playing basketball. Pushing off from the foot while the knee is straight, pivoting, jumping, and running are all movements that can overstretch the Achilles tendon and cause it to rupture. A rupture can also occur as the result of trauma that causes an over-stretching of the tendon, such as suddenly tripping or falling from a significant height. The Achilles tendon is particularly susceptible to injury if it is already weak. Therefore, individuals who have a history of tendinitis or tendinosis are more prone to a tendon rupture. Similarly, individuals who have arthritis and overcompensate for their joint pain by putting more stress on the Achilles tendon may also be more susceptible to an Achilles tendon rupture. Symptoms Symptoms of an Achilles tendon injury are as follows. Pain along the back of your foot and above your heel, especially when stretching your ankle or standing on your toes; with tendinitis, pain may be mild and worsen gradually. If you rupture the tendon, pain can be abrupt and severe. Tenderness. Swelling. Stiffness. Hearing a snapping or popping noise during the injury. Difficulty flexing your foot or pointing your toes (in complete tears of the tendon). Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment This condition should be diagnosed and treated as soon as possible, because prompt treatment probably improves recovery. You may need to be referred urgently to see a doctor in an orthopaedic department or accident and emergency department. Meanwhile, if a ruptured Achilles tendon is suspected, you should not put any weight on that foot, so do not walk on it at all.Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. The decision of whether to proceed with surgery or non-surgical treatment is based on the severity of the rupture and the patient?s health status and activity level. Non-surgical treatment, which is generally associated with a higher rate of re-rupture, is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. Non-surgical treatment involves use of a cast, walking boot, or brace to restrict motion and allow the torn tendon to heal.  Surgical Treatment Surgical techniques for rupture repair are varied but usually involve reapproximation of the torn ends of the Achilles tendon, sometimes reinforced by the gastrocsoleus aponeurosis or plantaris tendon. Open reconstruction is undertaken using a medial longitudinal approach. Studies indicate that patients who undergo percutaneous, rather than an open, Achilles tendon rupture repair have a minimal rate of infection but a high rate of sural nerve entrapment (16.7% of treated cases). Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy. Surgical Treatment Surgical techniques for rupture repair are varied but usually involve reapproximation of the torn ends of the Achilles tendon, sometimes reinforced by the gastrocsoleus aponeurosis or plantaris tendon. Open reconstruction is undertaken using a medial longitudinal approach. Studies indicate that patients who undergo percutaneous, rather than an open, Achilles tendon rupture repair have a minimal rate of infection but a high rate of sural nerve entrapment (16.7% of treated cases). Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy.
Comments are closed.
|
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
July 2017
Categories |
 RSS Feed
RSS Feed
